Generating and using scripted role-plays in the teaching of interpreting and language
INTRODUCTION
In response to undergraduate calls for more vocational modules for students of French at the University of Leeds, I designed a level-2 ‘Introduction to Professional Translation and Interpreting’ (IPTI). Students participate in role-plays throughout the year and so learn, through experience, observation, and feedback/discussion, the interpreting skills on which they are assessed.[i] In this article, we shall look at the rationale behind the use and form(s) of role-play in the teaching of interpreting. We shall explore the ideas that scripted role-plays ‘work’ better than semi- or unscripted scenarios, and that generating scripts is preferable to ‘borrowing’ existing scenarios. There will then follow some comments on how role-plays can be used in a 50-minute seminar. To conclude, we shall discuss more general benefits of using scripted role-plays in the teaching of foreign languages.
Role-play scenarios – whether scripted, semi-scripted, or unscripted – are used in a wide variety of pedagogical contexts (for example, see Alden, 1999; Schweickert & Heeren, 1999; Kettula & Berghäll, 2013). The principal reasons cited by non-linguists for using role-play in their teaching are that they:
- promote participation;
- enhance engagement;
- allow students to experience different perspectives.
In the case of teaching interpreting, as well as improving confidence in speaking skills, role-plays enhance other skills such as emotional intelligence, and can also be used to inform students about health issues.
In IPTI, the mode of ‘community interpreting’ (see below) is used: most scenarios involve a GP and a patient. Whichever mode is chosen, questions soon arise regarding the framing, composition, and presentation of the role-plays. For example, is it more realistic, and/or more beneficial for student learning, for the GP and patient not to be able to see each other’s lines? Is there anything to be said for providing scripts with both roles in English (and so expecting the GP, for example, to sight-translate his/her role)? How should students be expected to prepare for the role-plays?
The mode of ‘community interpreting’
Interpreting can take many forms. Without wishing to get embroiled in taxonomy, the mode chosen for this module is ‘community interpreting’ (CI). Roughly put, this can certainly be understood as distinct from simultaneous interpreting (but not necessarily from chuchotage) and can justifiably be seen as different to interpreting in the contexts of conferences, business, and the courts. Many understand CI as the relevant mode when enabling non-speakers of English, for example, to access services such as health and social care in the UK. [ii]
Choosing CI as the mode of interpreting for this level-2 module offers many advantages over other modes. In business interpreting, for example, it is common practice to interpret in the third-person. In CI, ‘Oui!’ would be rendered as ‘Yes!’ and not as ‘Madame Bovary agrees strongly with that.’ By reducing the amount of grammatical manipulation required, CI is arguably – and appropriately, at this level – easier to perform.[iii]
The style of CI is relatively informal. This makes any need to seek clarification or repetition less daunting.[iv] Moreover, whilst all students will have personal experience of seeking health advice, not all students will have experience of participating in formal conferences, business meetings, or legal proceedings. The context of CI is one to which all students can relate. This helps them to produce language that is appropriate, authentic, and meaningful in context.
A potential argument against the use of CI is that – in interpreting in the first-person – the interpreter ‘becomes’ the patient. This is recognised as a risk for interpreters working with patients with PTSD, for instance.[v] One solution is to avoid certain subjects that may be deemed either distressing or ‘near the bone’. Another solution is to teach students that refusing to interpret is a perfectly acceptable choice (see Hale, 2007: 150-51 & 157). The same would pertain where a student with strong religious beliefs or certain cultural traditions, for example, would be uncomfortable with role-playing in a situation involving ‘taboo’ subjects – for some – such as abortion. Empowering and encouraging students to make this decision – should they feel the need – itself improves assertiveness and raises professional awareness of ethics and codes of practice.
To script or not to script?
Scripts are not the only option. For some, ‘authentic spoken dialogues are the optimal teaching instrument’ (Rudvin & Tomassini, 2011: 140). Another ideal involves two teachers who ‘act as if they really need the services of the student interpreter’ (Sandrelli, 2001: 173-96). Hale discusses another ideal, which involves ‘service providers in classroom role-plays to provide authentic practical experience for both students and providers’ (Hale, 2007: 171). After a brief analysis of the suitability of these formats, we shall look at different ways of presenting scripted role-plays.
In the context of IPTI, using ‘authentic spoken dialogues’ would be unwieldy and impractical in the classroom. Moreover, interpreting disembodied voices cuts out the human: body language is sidelined, spontaneity is impossible. Moreover, what the dialogues gain in realism is arguably lost every time that the pause button is pushed. There is also the ethical issue of confidentiality to overcome – where would these ‘real-world’ recordings come from? Beyond that, and beyond the classroom, however, the format itself would work well as a complementary way for students to practise on their own (see Hansen & Shlesinger, 2007).
Having two teachers play roles for the benefit of one student at a time is again – in the context of IPTI – unfeasible. With small groups and at a higher level, perhaps, this format would work well. It certainly remedies the issue of spontaneity, as Sandrelli discusses (Sandrelli, 2001). In IPTI, however, it has the disadvantage of reducing opportunities for students to role-play and to see the interpreting process for themselves through the eyes of the doctor and patient.
A potentially more attractive alternative – whilst prey to the same issues as in having two teachers play the roles – is to involve real service providers. Establishing links with professional communities outside the university would be progressive and mutually beneficial, as Hale suggests. However, the barrier here might be financial or due to the workloads of such service providers. That said, if only one ‘real’ service provider were to participate somehow in one seminar per term/semester, all parties concerned would be enriched and gain new insights.
As for scripts, we cannot assume that all students in any given group will have the confidence, imagination, or knowledge to improvise a patient/doctor role from a skeletal (unscripted) scenario. Hale summarises the dilemma very well:
Scripted dialogues are useful for controlling content, grammatical structures and vocabulary, but unless they contain features of spoken discourse and are well acted out, they will sound stilted and artificial. On the other hand, unscripted dialogues, where actors are provided with a scenario to improvise, can be useful for spontaneity but may lack depth of content and richness of language. (Hale, 2007: 171).
Given that IPTI students will participate in some 18 role-plays in the course of the module, their (scripted) role-playing will evolve diachronically with practice and through routine. Scripted roles offer the advantage of enabling everyone – regardless of confidence or readiness to take risks – to participate in the scenarios, from the first to the last. They facilitate inclusivity. It could be argued that students are not assessed on their acting skills, imagination, or ability to improvise, and so should not be given this extra pressure during teaching. But improvisation and ‘Theoretical Theatre’ (in the form of unscripted role-play) are innovative and experiential teaching formats that could work well, with appropriate training and introduction (see Seyfang, Hargreaves, & Lorenzoni, 2017).
Some students embrace role-play with gusto. These students are not necessarily the ‘best’ – in terms of language production – but my hypothesis is that they will improve quickest, through being ready to ‘take risks’. Other students, on the other hand, may well laugh or even cringe at the invitation to ‘ham up’ the role of the patient. And these students – who may seem more shy or insecure – are not necessarily those with the least developed language skills.[vi] For me, inclusivity is a key factor and is best facilitated by scripted role-plays. Scripts also reduce the risk of the scenario coming to an embarrassing halt.
The fact that different triads perform the same (scripted) role-plays in the same seminar/session is also beneficial when it comes to feedback and discussion. Different translation strategies and solutions for particular (shared) problems will inevitably arise and so provide useful material – within the seminar/session – for comparison and reflection.
Semi- or unscripted scenarios are arguably better in terms of offering more realistic material – facilitating human contact and the naturalness of language, for example. Expecting students to improvise the roles of GP and patient, however, is quite demanding. It involves level-2 students coming up with the specialist language of a French-speaking doctor, asking questions and delivering content in a natural, convincing manner, and in a suitable register. This could potentially be overcome by giving the group three ‘complaints’ to research – before role-play – and so allowing students to prepare for their respective roles. I fear, however, that this might involve an inordinate amount of co-ordination.
A borrower be?
‘Borrowing’ or adapting pre-existing role-play scenarios that can be found online, for example, might appear to be an attractive, time-saving option. In my experience, however, material appropriate to borrow soon runs out. The quality of ‘free’ material – especially online – is frequently of a standard requiring much editing and correction, thus proving to be a false economy. Rudvin & Tomassini (2011) have paved the way in publishing good quality materials, but the volume of such material remains low.
Ultimately, I have found it more time-efficient to write my own scripts. Having chosen a medical setting for the role-plays, I mine relevant information by consulting France’s most popular online health site, Doctissimo. With a particular complaint in mind – say, insomnia – I will research realistic signs and symptoms for the role of the patient. The site also provides real advice and treatment which can be cannibalised for the role of the doctor. The logic and conventions of a GP appointment mean that there is, in a sense, a formula to follow, and this makes composition relatively easy.
Writing the scripts myself has enabled me to choose certain complaints for certain reasons. For example, potentially embarrassing or taboo subjects such as STDs can be broached in the role-play. From an interpreting point of view, this may represent a test of maturity, neutrality, and sang-froid. Linguistically, the challenge may be one of vocabulary. And given the average age of my students, the health advice contained in the role-play (and bolstered by the accompanying sight-translation) could serve their own well-being. Sadly, for example, depression is currently rife among students. For this reason, in the run-up to Christmas, I use a scripted role-play and sight translation on the subject of depression/SAD. For the sake of variety, other complaints have included: gastroenteritis, hypoglycemia, head injury, asthma, eczema, flu, stress, and stomach ache.
In writing the scripts, the tutor can ensure a balance between content that is relatively easy to translate and material that may prove more challenging. Idioms, proverbs, metaphor, and culturally-loaded language can be incorporated into the script in order to ensure that any unthinking word-for-word translation is exposed as inadequate. For example, in one scenario, the English-speaking patient says, ‘That’s a relief, doc! I thought it was my ticker!’ Many level-2 students may attempt to give an interlineal translation such as ‘C’est un relief, doc! J’ai pensé (que) c’était mon tiqueur!’ This rendering could give rise to all sorts of discussion and reflection:
- The French ‘relief’ only overlaps with the English ‘relief’ in the sense of ‘raised pattern’. The meaning is synonymous with ‘Phew!’ and so a more communicative translation might be ‘Quel soulagement!’ This raises the issue of ‘false friends’.
- For ‘doc’, students might be expected to raise the register in French (by rendering it as ‘docteur’), to match the formality of the setting.
- The simple past in English would not be rendered, here, with the passé composé in French – which is the tense that many level-2 students would choose (out of habit). Either the imperfect or pluperfect would be more idiomatic in French: ‘Je pensais / J’avais pensé.’
- The use of franglais could show a lack of understanding of the original – in which case, clarification should be sought. Alternatively, it exposes an inability to find a synonym or alternative rendering with the same meaning (for example, through transposition: ‘un problème cardiaque’). Rendering ‘ticker’ as ‘cœur’ is accurate, communicative, and appropriate in terms of register.
As we see, this compact intervention raises issues of lexis, register, grammar, and practice. They are examples of issues that students would be expected to tackle – should they arise – in subsequent discussion.
SCRIPTS: A CHOICE OF STYLES AND APPROACHES
If writing scripts is a tutor’s preferred choice – for reasons of time, space, money, logistics, practical organisation, and in view of different students’ needs and capacities – another question presents itself: how should the scripts be presented?
The EN-EN model[vii]
For reasons of expediency, I began by using scripts with both roles in English – EN-EN (see Figure 1): the target-language (TL) speaker is expected to sight-translate the role (EN>TL) on the spot. Sight-translation is another valuable skill that is developed by the module. However, if it is poorly executed, then this is not a fair challenge for the interpreter: the TL that is produced risks being inauthentic, unidiomatic, and unintelligible. It can be a case of ‘garbage in, garbage out’. With my level-2 students, who have typically not yet spent a term or year in a French-speaking country, the EN-EN model has not worked well. It might be best to drop this model and allow students to focus on one skill at a time: that is, strive for maximum realism in the interpreting exercises and practise sight-translation separately.
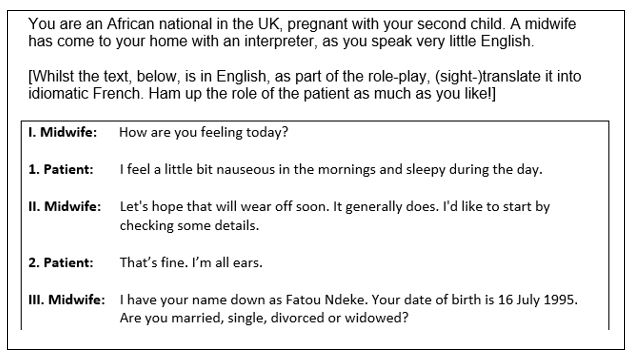
Figure 1: Sample of EN-EN script (IPTI course materials).
The temptation for the patient to translate too literally, or word-for-word, seems too great for most level-2 students – especially when they have the EN text in front of them. In this example, patients quickly run into trouble when faced with the adjectives ‘nauseous’, ‘sleepy’ and the expression ‘to be all ears’. If they come up with ‘nauséeuse’, ‘endormie’, and ‘être tout(es) oreille(s)’, there is in fact every chance that the interpreter will translate these correctly – that is, as the intervention reads in the original EN. However, this is not helpful in interpreter training or language learning: it exposes the interpreter to TL that is neither authentic/idiomatic or of appropriate register. Nor does it demand the same dexterity or ability to re-phrase the TL into idiomatic EN.
The EN-TL model
A more ‘realistic’ way to present the script is with one EN role and the other as a TL role. Some of my role-plays are set in the UK, so the doctor’s role is in English and the role of the patient (whether a francophone tourist or asylum-seeker) is in French. This can be flipped (see Figure 2). The EN-TL model ensures that the TL (French, in this case) is correct, idiomatic, and suited to the level.[viii] This allows the francophone role-player to concentrate on his/her accent, pronunciation, and intonation. More importantly, perhaps, this represents a fairer challenge to the interpreter.
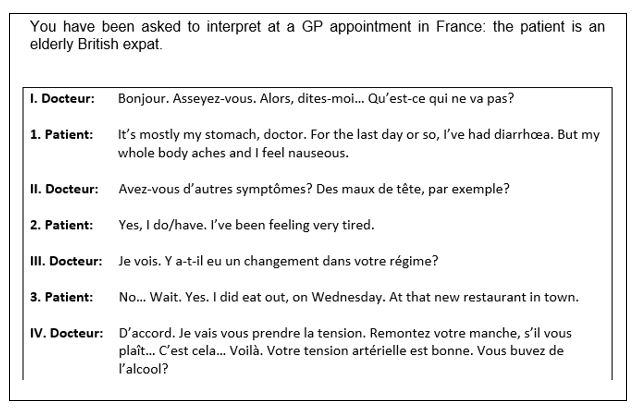
Figure 2: Sample of EN-TL script (IPTI March exam, 2017).
Note that some elements of contextual awareness can be written into the scenario. Whether the patient replies, ‘Yes, I do’ or ‘Yes, I have’ depends on how ‘Avez-vous..?’ is interpreted: ‘Do you have..?’ or ‘Have you got..?’ Also note that features of spoken language – hesitation, self-correction – can be written into the scripts by the tutor. Such features keep the role-players on their toes.
The EN/TL (unseen) model
In the EN-TL and EN-EN models discussed above, the GP and patient can see each other’s lines. This maximises contextual understanding and provides an opportunity for them to assess the performance of the interpreter. However, a disadvantage of this format is that they can too easily be tempted to focus on the page. This hinders eye-contact and makes body language awkward. One remedy for this is to provide the GP and patient with EN-unseen and TL-unseen scripts, respectively (see Figures 3a & 3b).
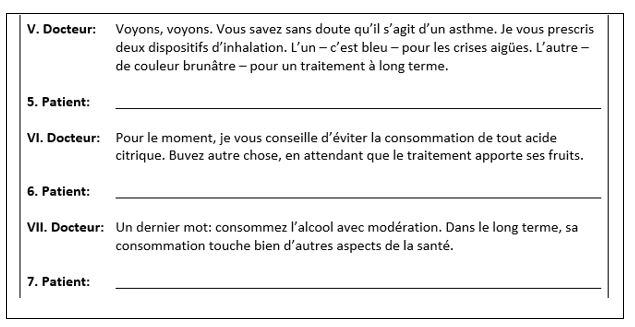
Figure 3a: Sample of TL-unseen script (IPTI course materials).
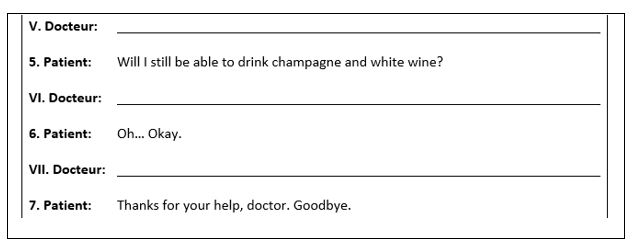
Figure 3b: Sample of EN-unseen script (IPTI course materials).
When the patient (reading), for example, is answering the doctor’s question, the doctor cannot see the patient’s text and is more inclined to look at the patient and listen to what s/he is saying. When it comes to the interpreter to relay what the patient has said, the doctor cannot ‘follow’ the text on the page: s/he will therefore be more likely to make eye contact with the interpreter and will have to rely on his/her own memory in order to gauge the quality of the interpreting.
In my experience, EN/TL (unseen) has proven to be the students’ preferred format. Roles and tasks are clear and achievable and the scenario ‘flows’ more smoothly:
- the EN patient can focus on playing the patient, has also to listen to the doctor’s TL, and so can assess the quality of interpreting;
- the TL doctor can read the script in French, focusing on pronunciation and delivery, but also has to listen to the patient for information, and is thus able to assess the quality of interpreting;
- the interpreter is guaranteed to hear good quality language to interpret (both EN and TL) for a doctor and patient who will be listening to – and not following on the page – what is being said.
Realism in this form of role-play is an aspiration – up to a point – but it is not an end in itself. Students seem naturally to embrace the ‘playful’ aspect more than trying to be realistic. This is a timely reminder of the importance of enabling students to role-play.
Alternative scenarios
In the name of variety, I have also experimented with other ways of generating role-plays. For example, I based one dialogue on ‘Doctor, doctor’ jokes (see Figure 4). Humour – as we know – is difficult (and sometimes impossible) to translate. To be fair to the interpreter, the ‘Doctor, doctor’ jokes incorporated into the script had to be translatable. Thus, perhaps the most famous (‘– I feel like a pair of curtains… – Well, pull yourself togther.’) was rejected, as the English idiom has no obvious equivalent in French. Watching different triads role-play this scenario was very revealing. Some students – in whichever role – did not get the joke(s) at all. Typically, all role-players would eventually understand the logic behind the scenario and the interpreter would consciously ensure that the ‘punchlines’ made sense. Success, in this case, was gauged by groaning/laughter.
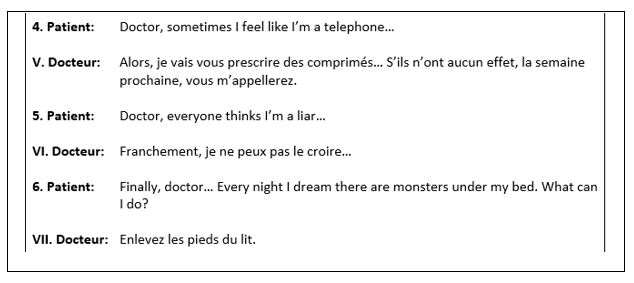
Figure 4: Sample of ‘Doctor, doctor’ script (IPTI course materials).
An even quicker way to generate pages of material is to find a decent translation (whether EN-TL or TL-EN) of a play.[ix] I have experimented with a translation of Ionesco’s La Cantatrice chauve (The Bald Prima Donna). I selected two scenes that represented a tough test – because confusing and amusing (see Figure 5). In the real world, we do not always understand the logic behind an utterance or the way in which it is phrased. Example: when interpreting, once, with a solicitor and her client (a refugee), the solicitor seemed to snap and adopt an almost rude, aggressive tone. My interpretation switched accordingly to a similar – if not quite so forceful – tone, though I did not know why the solicitor had done this. I had a word with her, after the meeting was over. She explained that her choice had been measured and deliberate: she wanted to provoke the client into providing more detailed evidence for her case – which she obtained. It was a case of being cruel to be kind.
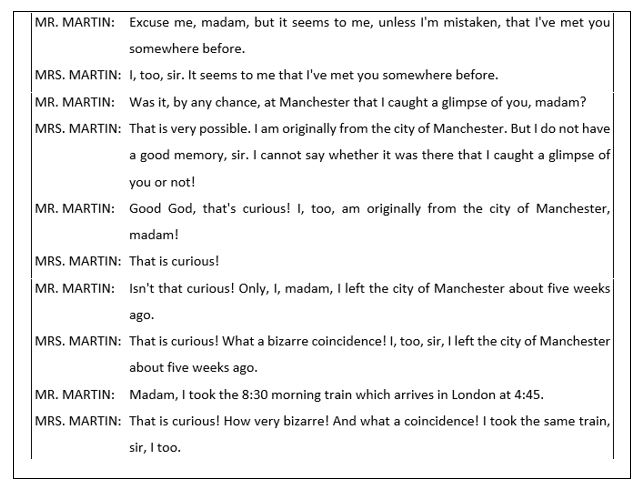
Figure 5: Sample of Theatre script – EN role (IPTI course materials).
In interpreting this nonsense, students learn to translate what they hear – not what they think they should hear. With the suspension of common sense and logic, students have to listen very carefully and remain calm and professional, though the situation is absurd.
A TYPICAL SEMINAR
Effective interpreting depends on good language skills (listening/comprehension, the ability to re-phrase/re-formulate), note-taking/memory, and preparation (of vocabulary and contextual understanding). For Simpson, ‘role-play has three phases: preparation, interaction, and discussion’.(Simpson, 1985: 77). One way of helping students prepare for the scenarios is to give them ‘vocab lists’. These can be presented as glossaries – with the EN-TL translation – or as a list of English terms, solely, requiring translation/research. For the exam, students are given a keyword.
Ideally, therefore, all 12 students will arrive at the seminar having done their research and having learned relevant vocabulary. Splitting into four triads, and moving – physically, say, to the corners of the room – so as to maximise the space (for reasons of noise/interference), students may be asked to re-cap on the skills, tools, and approaches that they are learning. For example: note-taking, ‘leaving the Ego at the door’, avoiding ‘ADO’ (addition, distortion, omission), maintaining eye contact, and being free to seek clarification. Each triad will decide which member is playing which part and is then given two scripts: one for the GP and one for the patient. The triads are then left to get on with the role-play. My approach, as tutor, is to listen – unobtrusively – to the different triads with the aim of spotting examples of good and bad practice. For each role-play, students are encouraged to:
- give feedback to the interpreter on his/her performance;
- focus on linguistic issues that proved challenging;
- discuss alternative strategies/solutions for said issues.
As each triad will work at a different pace, it is up to the tutor to be alert and ensure that this model is repeated three times – within the seminar/session – so that each member of each triad has the opportunity to play each of the roles. Time should be left at the end of the three role-plays for group discussion and reflection.
Student attendance cannot, however, be guaranteed. The tutor, therefore, must be willing to step into the breach, if one triad – for example – is short of a member. Sometimes, the only answer in the face of absentees – depending on numbers – is to ask certain students to work in couples. This can be very confusing for them – certainly initially – and is most unrrealistic. But the students that I have observed in such circumstances have adapted surprisingly well – and some even prefer to work in this way.
Before the group has bonded, it may be that peer feedback verges on the trite. Students are often wonderfully supportive of each other, offering unreserved praise and congratulations on a ‘great performance’. That said, feedback will typically evolve – to be more critical (constructive/reflective) – and students are more than able to identify challenges and discuss possible strategies/solutions. Group discussion, at the end of the seminar, is an opportunity for the tutor – armed with examples gleaned from eavesdropping – to lead further discussion on particular issues and encourage critical thinking.[x]
CONCLUSION
IPTI was designed as a ‘taster’ for students interested in professional translation and interpreting. Few – if any – of the students on this module may ever practise professionally as interpreters. What has stood out, however – from what I have observed and learnt from student feedback – is that:
- IPTI (level-2) students are very keen to use their TL;
- students see interpreting as a challenge;
- through practice/role-play, students gain better understanding of certain aspects of translation theory.
Having never – typically – spent a term/ year in a French-speaking country, their confidence in speaking, in particular, may be at a low, given that they are still concentrating on grappling with grammar and building vocabulary. With a framework for acquiring vocabulary (the glossary), an understanding of the dangers of faux amis (through research), and being regularly obliged to use their EN/TL language skills (in a scripted role-play), students have ample opportunity to use the TL. Through practice (of speaking and listening), students learn where their TL weaknesses lie: whether in certain aspects of grammar (for example, choice of tense) or, more generally, in their ability to paraphrase (through re-formulation, re-structuring, or translating ‘phrase function rather than structure’ – see Armstrong, 2005: 120).
Interpreting is certainly a challenge. It exposes the interpreter’s ability in both languages, demands professionalism, understanding of ethics, as well as preparation/research, and is physically and mentally demanding. In addition to language skills, it requires stamina, emotional intelligence, empathy, resilience, and (quick) lateral thinking. Learning about the theory and practice of interpreting and practising interpreting skills, I should argue, is a win-win for students. It helps them to decide whether interpreting is for them, career-wise, whilst enabling them to improve the above qualities and skills.
The process of interpreting is itself beneficial more generally to language acquisition and understanding how languages ‘work’ – in context. Students make more of an effort to avoid word-for-word translation (especially TL>EN) in an interpreting setting – with their peers – than they would in writing. When the language is serving a tangible purpose – for example, getting a patient to roll up his/her sleeve – the success of interpreting can be gauged immediately. Students quickly learn the importance of paraphrasing – if only to save face.
With its stock of prefixes and suffixes, medical language is useful in enabling students to discern ‘patterns’ (for example: appendicite, dermatite, hépatite, méningite, thrombophlébite). It also exposes unfathomable cultural differences in the usage of French and English. For example, the impersonal French structure (J’ai mal à la jambe, ‘I have pain/ache in the leg’) in contrast with the English structures: ‘My leg hurts’, ‘I’ve (got) a pain in my leg’. Another cultural difference concerns register. For example, the highly technical arcade sourcilière (‘superciliary arch’, ‘supraorbital arch/ridge’) is used commonly in France. In everyday English (and at the GP’s), this is simply the ‘eyebrow’.
In conclusion, scripted role-plays might have their drawbacks but they present many advantages. For students, scripted (CI) role-play scenarios:
- minimise stress and maximise inclusivity;
- build confidence in performing the interpreter’s role and in speaking, generally;
- allow them to understand the interpreting process –reflectively – from three angles;
- involve risk-taking (in a safe environment) which can be fun/exciting/challenging;
- can have a positive impact on students’ well-being and awareness of health issues;
- improve understanding of grammar;
- improve knowledge of vocabulary – including specialised vocabulary;
- serve to help prepare students for their term/year abroad.
For tutors, generating and using scripted role-plays affords:
- a chance for the tutor-cum-playwright manqué to design and control the content of the learning material;
- the possibility to tailor language complexity according to level;
- an opportunity to include information that will be beneficial to students in view of their term/year abroad and general health/well-being.
REFERENCES
Alden, Dave, ‘Experience with Scripted Role Play in Environmental Economics’, in Journal of Economic Education, Spring (1999), 127-32.
Armstrong, Nigel, Translation, Linguistics, Culture: A French-English Handbook, (Clevedon: Multilingual Matters, 2005).
Berthold, S. Megan & Fischman, Yael, ‘Social Work with Trauma Survivors: Collaboration with Interpreters’, in Social Work, Vol. 59 Issue 2 (2014), 103-110.
Gorm Hansen, Inge, & Shlesinger, Miriam, ‘Technology and self-study in the interpreting classroom’, in Interpreting, Volume 9 No 1 (2007), 95-118.
Hale, Sandra Beatriz, Community Interpreting, (Palgrave Macmillan: London, 2007).
Kettula, Kirsi & Berghäll, Sami, ‘Drama-based Role-play: a Tool to Supplement Work-based Learning in Higher Education’, in Journal of Workplace Learning, Vol. 25 Issue 8 (2013), 556-75.
Lor, Mailee, ‘Effects of Client Trauma on Interpreters: An Exploratory Study of Vicarious Trauma’, in Master of Social Work Clinical Research Papers. Paper 53 (2012). <http://sophia.stkate.edu/msw_papers/53>. [Accessed: 18/07/2017.]
Mikkelson, Holly, ‘Interpreting is Interpreting – or is it?’ GSTI 30th Anniversary Conference (1999). <https://works.bepress.com/holly_mikkelson/9/>. [Accessed: 18/07/2017.]
Rudvin, Mette & Tomassini, Elena, Interpreting in the Community and Workplace: A Practical Teaching Guide, (Palgrave & MacMillan: London, 2011).
Sandrelli, Annalisa, ‘Teaching Liaison Interpreting: Combining Tradition and Innovation’, in Triadic Exchanges: Studies in Dialogue Interpreting ed. by Ian Mason (Manchester: St Jerome Publishing, 2001), 173-96.
Schweickert, Eileen A. & Heeren, Allison B., ‘Scripted Role play: a Technique for Teaching Sexual History Taking’, in Journal of the American Osteopathic Association, Vol. 99 No 5 (1999), 275-76.
Seyfang, Gill, Hargreaves, Tom, & Lorenzoni, Irene, Comedy in the Classroom: Innovative Teaching in Higher Education, Using the Performing Arts to Engage and Inspire Students (2017). <https://comedyintheclassroom.org/> [Accessed: 18/07/2017].
Simpson, Michael A., ‘How to Use Role-Play in Medical Training’, in Medical Teaching, Medical Teacher, Volume 7 No 1 (1985), 77.
Address for correspondence:
FOOTNOTES
[i] In semester 1, students submit a portfolio (including a glossary and reflection). In semester 2, assessment is based on a 10-minute exam consisting of an interpreting role-play and sight translation.
[ii] Some writers would include ‘court interpreting’ in their definition of ‘community interpreting’. See Holly Mikkelson, 2017.
[iii] Oddly, however, this appears to be counter-intuitive to students, who will typically begin interpreting with the frame of ‘S/He’s just said…’
[iv] Before role-playing, students are taught to ‘Leave the Ego at the door’. Briefly, this means not ‘blagging’ or ‘bluffing’. Students are encouraged to seek clarification when they have not understood/heard something or if their notes/memory mean that they have forgotten something.
[v] Identifying with a patient with PTSD can have an adverse effect on the interpreter. For example, see Lor, 2012; Berthold & Fischman, 2014.
[vi] Interpreting is a great leveller. In training students, the tutor may well see pride come before a fall – in the over-confident student – and tears from the quiet perfectionist.
[vii] I first devised scripts to teach CI to groups of adult learners with various languages: it was not uncommon for one group to be made up of speakers of TLs as diverse as Chinese, French, Hindi, Hungarian, Italian, Mirpuri, Pashto, Polish, Slovenian, Thai, Urdu, and Vietnamese. Producing EN-TL scenarios for each language was understandably unthinkable (for innumerable practical reasons).
[viii] Whilst I write both parts, as a non-native speaker of French I always have the text checked by a colleague who is a native speaker of French. This ensures that the language is accurate, idiomatic, and appropriate.
[ix] In this way, each triad can work with one TL version and one EN version.
[x] Hale has listed myriad aspects – or ‘points of departure’ – that may be prompted by role-plays for ‘discussions on language- and communication-related features’. See Hale, 2007: 141.